
 Elaine, a 1 year old spayed female Domestic Shorthair Cat presented on an emergency basis for a peracute onset of severe vestibular dysfunction which improved rapidly over several hours. Her family awoke to her hissing, she was found hiding, had an increased respiratory effort, vomited, and was falling/rolling. On presentation to PVESC’s Emergency Service, Elaine had horizontal nystagmus with the fast phase to the left, a right head tilt, and was attempting to circle to the right but was non-ambulatory. Within 2-3 hours, her only residual sign was a mild head tilt to the right. Elaine has no previous history of vestibular dysfunction or ear disease. She had otherwise been healthy, though had always been a small kitty.
Elaine, a 1 year old spayed female Domestic Shorthair Cat presented on an emergency basis for a peracute onset of severe vestibular dysfunction which improved rapidly over several hours. Her family awoke to her hissing, she was found hiding, had an increased respiratory effort, vomited, and was falling/rolling. On presentation to PVESC’s Emergency Service, Elaine had horizontal nystagmus with the fast phase to the left, a right head tilt, and was attempting to circle to the right but was non-ambulatory. Within 2-3 hours, her only residual sign was a mild head tilt to the right. Elaine has no previous history of vestibular dysfunction or ear disease. She had otherwise been healthy, though had always been a small kitty.
Elaine’s initial neurologic examination localized her signs to right-sided vestibular dysfunction without any central vs peripheral differentiating signs. Differentials for her signs included middle/inner ear disease (polyp/mass vs infection), idiopathic, vascular event/stroke, infectious diseases, auto-immune inflammatory conditions, metabolic conditions, cancer, etc.
Further testing as well as monitoring for any change in her condition given her rapid improvements were discussed and it was opted to perform additional testing. Blood pressure evaluation was within normal limits as was complete blood work (including ammonia, creatinine kinase, and globulins. Thoracic and abdominal radiograph were performed which revealed an undulant capsule margin at the cranial pole of the left kidney which could be seen with a congenital renal cyst, lymphoma, feline infectious peritonitis, or other granulomatous lesions. Abdominal ultrasound showed bilateral renal rim sign which was suggestive of an inflammatory condition such as FIP, pyelonephritis, or primary glomerulonephritis.
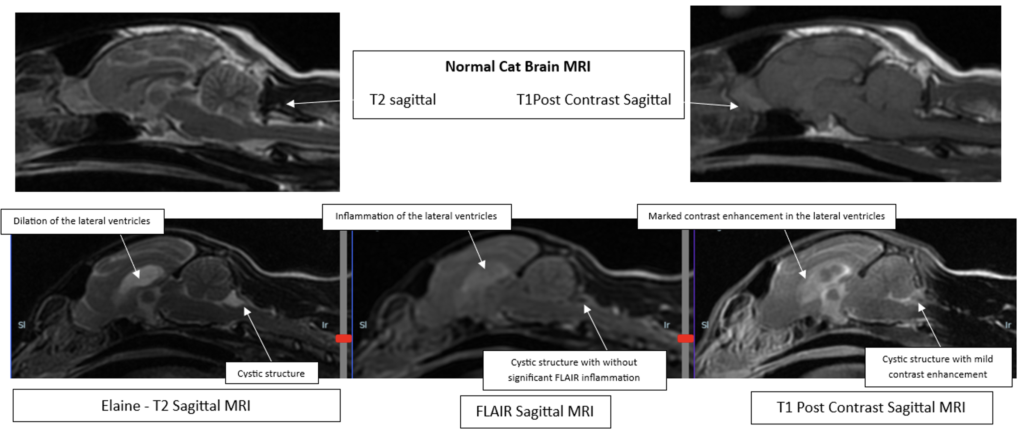
An MRI was then performed which revealed several abnormalities including meningitis, ventricular inflammation (ependymitis), encephalitis, moderate hydrocephalus, and bilateral anterior uveitis. The primary differential for all of Elaine’s kidney, brain, and eye changes was feline infectious peritonitis (FIP). There was also a small area of CSF fluid accumulation along the caudal fossa without significant mass effect which was suspected to be an incidental arachnoid cyst. Given the likelihood of FIP, BOVA (GS-441524) as well as clindamycin while awaiting pending test results.
Infectious disease testing confirmed that Elaine’s Feline Coronavirus (FeCV) titer was markedly elevated at >/= 1:12,800. An end-point titer was discussed but not pursued. She was also found to be moderately positive for Ehrlichia at 1:80 which could have been due to previous exposure or early infection. The remainder of Elaine’s infectious disease test results were negative (titers for Lyme, anaplasmosis, Rocky Mountain Spotted Fever, FeLV, FIV, toxoplasmosis (IgG & IgM), and cryptococcus).
Treatment with BOVA (GS-441524) was continued and if there was any worsening, then consider adding doxycycline. Omeprazole was prescribed to help decrease CSF production given the likely obstructive hydrocephalus. BOVA dosing was 10 mg/kg (25 mg) PO every 12 hours for 12 weeks.
Oral dosages vary depending on the form of FIP:
- 15 mg/kg/day for wet or dry FIP that does NOT have ocular or neurological involvement
- 20 mg/kg/day for ocular FIP
- 10 mg/kg q12hr (20 mg/kg/day) for neurological FIP
- Some cats may benefit from the dose being divided into 12 hour dosing to optimize the serum levels of GS.
Subcutaneous (injection) dosages:
- 6-7.5 mg/kg for wet and dry FIP that does NOT have ocular or neurological involvement
- 10 mg/kg for ocular FIP
- 10 mg/kg (minimum) for neurological FIP
Bova generally has mild side effects which could include stomach upset (nausea, drooling, diarrhea), lethargy, elevations in liver enzymes, elevation in kidney values, and bladder stones.
Elaine did very well with treatment with BOVA and became more active and inquisitive. Her appetite also improved significantly. At the time of her most recent recheck evaluation 4 weeks following initiation of treatment, her neurologic examination was normal.
Cats with the neurologic form of FIP can present with a variety of different signs. Cerebellar and vestibular signs are not uncommon as FIP causes production of immunoglobulins in the brain which can result in obstructive hydrocephalus particularly at the level of the 4th ventricle at the level of the cerebellovestibular system. What was unusual in Elaine’s case was how peracute the onset of her signs was and how rapidly she improved without any intervention. The additional finding of an arachnoid cyst is also an interesting though likely incidental finding which made initial interpretation of her MRI findings challenging. This could be monitored with serial MRIs in the future.
We are hopeful that Elaine will continue to do well with a 12 week course of BOVA. Some patients with the neurologic form of FIP do require more prolonged therapy. Monitoring for a decreasing FeCV titer as well as repeating an MRI could be beneficial in determining if more prolonged treatment is necessary.
Authored by: Danielle Eifler, DVM, Diplomate of the American College of Veterinary Internal Medicine, Specialty of Neurology, Certified Veterinary Neurosurgeon