A 9 yo MN DSH initially presented to PVESC Emergency Department in September 2025 for further evaluation of a decreased appetite. He had historically been managed with the PVESC Internal Medicine Service for a variety of comorbidities, including feline chronic enteropathy, previous bouts of antibiotic responsive cholangiohepatitis, and feline lower urinary tract disease. On presentation to the ER, he was noted to have severely lipemic serum in addition to hyperglycemia and glucosuria with borderline acidosis but no ketosis. He was subsequently diagnosed with diabetes mellitus. He was treated with IV fluid therapy, insulin, ondansetron, potassium supplementation, and other supportive therapies. Additionally, due to his fractious nature in hospital, he required heavy sedation for any diagnostics and received dexmedetomidine and butorphanol as initial sedation as well as propofol as needed for further handling and diagnostics. Regarding his IV fluid therapy, he was given an initial ~13.5 mL/kg bolus over 1 hour and then maintained on 36 mL/hr (5 mL/kg/hr; twice maintenance) for 6 hours. This was then reduced to 27 mL/hr (4 mL/kg/hr) for 15 hours. Once he was noted to be consistently eating on his own, he was discharged to the owners for continued monitoring and management of his newly diagnosed diabetes.
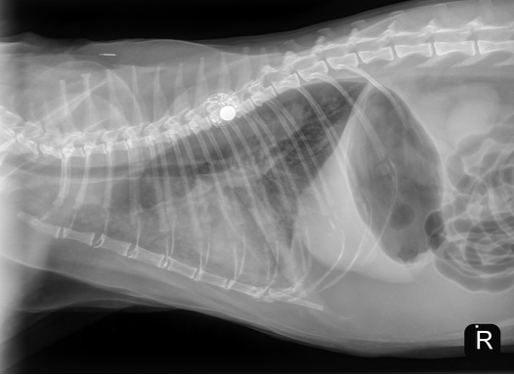
Unfortunately, the patient represented to the PVESC ER the day after discharge, for dyspnea, drooling, and frothing as well as an expiratory wheeze. On presentation he was given a 2 mg/kg dose of furosemide IM as well as butorphanol and alfaxalone for sedation to complete initial diagnostics. Thoracic radiographs on intake showed a mild cardiomegaly, moderate patchy interstitial pattern, and mild pleural fluid (see below). He was continued on 2 mg/kg furosemide IV (received two total doses approximately 4 – 6 hours apart). Later that day, an echocardiogram was performed which showed mild to moderate diffuse left ventricular concentric hypertrophy and only high normal left atrial size. The size of the left atrium was unexpected for the degree of pulmonary edema present on radiographs. At the time it was suspected that the patient likely experienced congestive heart failure secondary to fluid intolerance with underlying cardiomyopathy. Naturally occurring congestive heart failure (meaning congestive heart failure secondary to natural progression of feline cardiomyopathy) was considered less likely given the normal to minimally enlarged left atrial size (however, it could not be fully ruled out). The patient was discharged in the evening with oral medical management (furosemide, clopidogrel, and spironolactone) as he experienced significant stress in hospital and his respiratory rate and effort had improved significantly since presentation without the need for continued oxygen supplementation.


On recheck exam approximately 2 weeks later, the patient was doing clinically very well at home with resting respiratory rates around 28 breaths/min. Due to the increased stress that he experiences in hospital and the need for heavy sedation to perform any imaging, no additional thoracic radiographs were performed at this time. He was continued on his previously prescribed cardiac medications. Then, approximately 3 months later, he was rechecked again. At this visit, a recheck echocardiogram was performed which showed now normal left atrial size and mild LV concentric hypertrophy (overall significantly improved in comparison to previous). He was clinically doing very well at home with resting respiratory rates at home remaining at < 30 breaths per minute. Given the improvement in left atrial size and clinical improvement at home, the suspicion for fluid intolerant congestive heart failure increased. It was therefore elected to attempt a taper off some of his cardiac medications with eventual discontinuation of both the furosemide and spironolactone. As of a most recent update, the patient continues to do very well at home with stable resting respiratory rates and is now no longer receiving furosemide or spironolactone. Clopidogrel was continued at this time, however, it may be discontinued at a future recheck if the patient’s left atrial size remains normal.
The purpose of this case presentation is to highlight the importance of acknowledging the risk of fluid overload in middle to older age cats (with or without known cardiomyopathy), particularly since the long-term prognosis may be improved when compared to cats that experience naturally occurring congestive heart failure. Many cats that experience congestive heart failure secondary to fluid overload/fluid intolerance, after appropriate initial diuretic and supportive therapy, can be tapered off some or all their cardiac medications after several months. Echocardiography or repeat thoracic radiography are key for continued monitoring as improvement in cardiac structure and function is an important prognostic indicator and can be helpful in increasing suspicion for fluid intolerance/overload versus naturally occurring congestive heart failure. Please do not hesitate to reach out to PVESC’s Cardiology Service for help answering additional questions and discussing the best course of action for patients with congestive heart failure and heart disease.
Authored by: Eline Nijveldt, DVM, DACVIM (Cardiology)