 Opal is a 1.5 year SF Pit Bill Mix who presented to our Neurology service for a one-week history of dragging her pelvic limbs intermittently. Opal first started showing symptoms after running in the woods with her housemates. That evening she began limping in her pelvic limbs, and since then Opal had been only able to walk about 30 feet before she would start to drag her pelvic limbs behind her. Her owners report that with a period of rest she is able to get up in her back legs to attempt to walk again. Over the past few days she developed diarrhea and has not been eating well. A CBC, 4DX, and radiographs of the abdomen/thoracolumbar spine were unremarkable at the emergency veterinary hospital. Due to concern for back pain she was started in carprofen, methocarbamol, metronidazole, and gabapentin which did not improve her signs.
Opal is a 1.5 year SF Pit Bill Mix who presented to our Neurology service for a one-week history of dragging her pelvic limbs intermittently. Opal first started showing symptoms after running in the woods with her housemates. That evening she began limping in her pelvic limbs, and since then Opal had been only able to walk about 30 feet before she would start to drag her pelvic limbs behind her. Her owners report that with a period of rest she is able to get up in her back legs to attempt to walk again. Over the past few days she developed diarrhea and has not been eating well. A CBC, 4DX, and radiographs of the abdomen/thoracolumbar spine were unremarkable at the emergency veterinary hospital. Due to concern for back pain she was started in carprofen, methocarbamol, metronidazole, and gabapentin which did not improve her signs.
On neurological examination, Opal was bright and alert but nervous. When she rose from rest, she would walk 5-6 steps before she became progressively weak in the pelvic limbs, bunny hopped, and then collapsed in the forelimbs as well. After a minute of rest she would repeat this gait, until she collapses in all four limbs. Videos have been provided below. Cranial nerve examination was unremarkable, except for a fatiguing palpebral reflex. Her conscious proprioception was unremarkable in all four limbs, as were all her spinal reflexes. No pain was found on cervical range of motion or deep thoracolumbar and sacral spine palpation. Dr. Landry neuro-localized her to the neuromuscular junction. At her appointment thoracic radiographs, CBC/chemistry, and a T4 were unremarkable. Abdominal ultrasound was consistent with her recent colitis but was otherwise unremarkable. Due to the concern for myasthenia gravis, an acetylcholine receptor antibody titer (AChRAb titer) was submitted and Opal was started on pyridostigmine bromide.
This first video shows Opal’s gait after allowing her to rest in sternal recumbency for several minutes.
This second video shows Opal after we asked her to continue to walk following rest. The progression of pelvic limb weakness over multiple steps to bunny hopping and then collapse is typical of myasthenia gravis in dogs.
CLINICALLY RELEVANT FACTS:
- Acquired myasthenia gravis is an autoimmune condition in which there are autoantibodies made to the acetylcholine receptors at the neuromuscular junction. In some cases this may be paraneoplastic (secondary to a thymoma or other type of cancer), so thoracic radiographs and abdominal ultrasound are recommended. Dogs with paraneoplastic myasthenia gravis will not resolve spontaneously, and referral for removal of the tumor is often recommended. Thoracic radiographs are also recommended in order to screen for megaesophagus, as this is considered a common condition in dogs with myasthenia gravis which require elevated feedings and sometimes medications in order to avoid regurgitation and aspiration pneumonia.
- There are a small percent (previously reported to be 2%) of myasthenic dogs that are seronegative (have a negative or low titer). False positives are extremely rare. These dogs should be retested one month later, as some of them will convert and have a positive titer on recheck. There are several theories regarding seronegative myasthenia gravis, most common being that some dogs have autoantibodies against receptors on the NMJ end plate OTHER THAN acetylcholine (like titin or ryanodine receptors).
- Pyridostigmine bromide is an “anti-acetylcholinesterase” medication which, by inhibiting the acetylcholinesterase enzyme from breaking down acetylcholine, increases the bioavailability of acetylcholine and therefore increases the ability of nerve impulse transmission at the neuromuscular junction. This will clinically improve dogs with myasthenia gravis, but dogs with other neuromuscular junctionopathies can also improve clinically. Therefore a AChRAb titer should be submitted regardless of clinical improvement.
- Treatment should be continued until there is seroconversion of the AChRAb titer. The high risk of aspiration pneumonia has lead to the previously reported 50% one year mortality rate. However spontaneous remission has been reported in 80% of dogs within 6-8 months of diagnosis.
- Some cases will fail pyridostigmine bromide medication alone, and require the additional of immunosuppressive medications.
- Besides the hallmark appearance of their gait, dogs with myasthenia gravis will often have normal spinal reflexes and a fatiguing palpebral reflex.
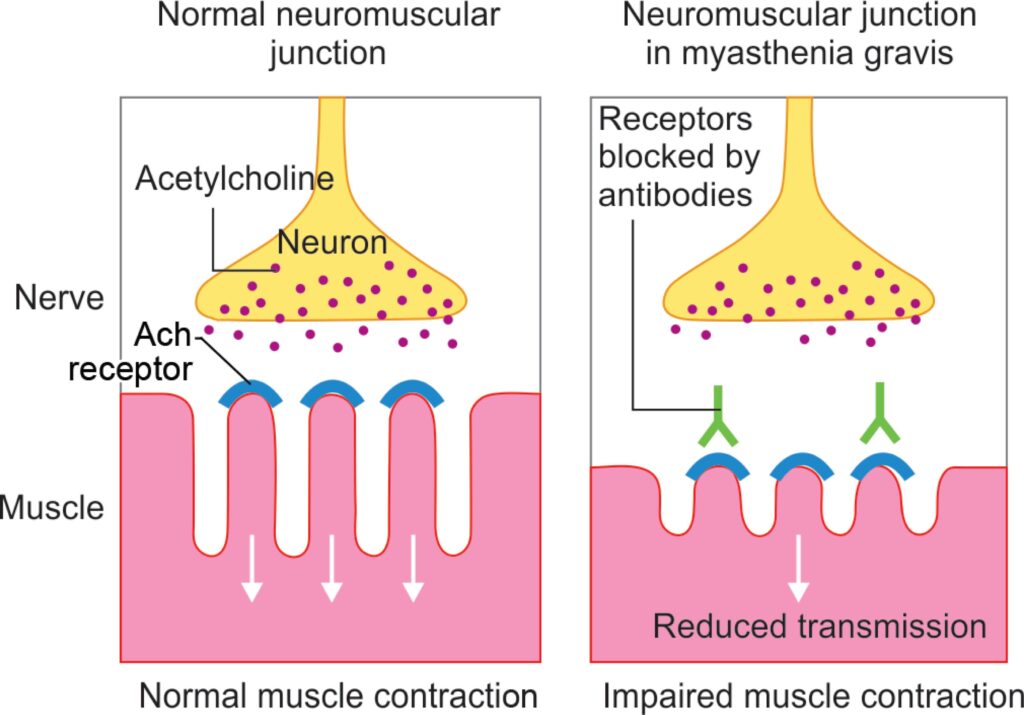
The normal neuromuscular junction vs the neuromuscular junction in a canine with myasthenia gravis. The patient with myasthenia gravis has acetylcholine receptors which are unusable as they are bound by autoantibody. These patients have limited neuromuscular transmission at these junctions and are clinically weak with exercise.
Authored by: Dr. Landry, DVM, DACVIM, Neurology